
Genu valgum is one of the most common reasons for pediatric orthopedic evaluation (“my child has knock knees”). The child presents with two lower limbs that “touch” at the knees and separate immediately below the knees, unlike genu varum (see related fact sheet).
In most cases, these are actually physiological conditions for which reassurance to the parents is sufficient. However, it is important to have a clear idea of which cases require greater attention and possible treatment.
The physiological development of the knee in children
It is essential for the pediatrician to understand the physiological development of the knee joint. Typically, newborns’ lower limbs exhibit a slight varus joint. This varus usually peaks around the time infants begin to stand, causing concern on the part of their parents.
Physiologically, the joint then tends to improve, reaching a neutral joint around 18–24 months. Subsequently, however, the joint continues to develop toward valgus, which peaks around 3.5–4 years of age; finally, the valgus joint decreases again and gradually returns to the mild physiological valgus of the adult knee.
When should you seek orthopedic advice for knock knees?
Some elements should make you require an orthopedic visit:
- Significant valgus: above certain numerical values, generally above 6-8 cm, especially if the physiological peak phase (4 years) has been exceeded.
- Asymmetry: one knee is much more valgus than the other
- Length difference: a valgus deformity present only in a shorter limb may hide a mild femoral hypoplasia
- Positive history of trauma, infections, etc.
- Physical examination for features suggestive of secondary valgus (e.g., rickets, etc.)
Idiopathic and secondary genu valgum
Idiopathic genu valgum
Some children, after the physiological development of the knee axis is complete (i.e., after about 8 years of age), continue to exhibit excessive genu valgum, even in the absence of underlying pathologies. This can lead to problems, particularly: difficulty walking and running (with the knees constantly rubbing together), patellar dysfunction (which “works poorly” due to the altered axis), and medial ligament laxity, in addition to the often-complained aesthetic concerns. Furthermore, if left untreated, over time it can lead to excessive overloading, resulting in cartilage wear on one side of the knee (the lateral side) compared to the other.
It is often found in hypotonic, overweight individuals, and is often associated with flat feet (see related fact sheet).
Secondary genu valgum
In this case, knock knees are due to an underlying condition. It’s essential to understand these possibilities so you can investigate and rule them out during the evaluation, and to request further investigation if you suspect something is wrong.
Some examples include:
- Rickets . This is one of the most common forms, and it is the one that must be investigated most carefully (both deficiency and genetic forms).
- Mild hypoplasia of the femur (congenital short femur, see related fact sheet) with hypoplasia of the lateral condyle causing valgus of the knee.
- Post-traumatic valgus : following a compound fracture of the proximal tibia, the onset of knee valgus, which has a characteristic pattern, may occur over time; or following injury to the growth plate (consequent to epiphyseal detachments of the distal femur or proximal tibia).
- Skeletal dysplasias : metaphyseal, spondyloepiphyseal, etc.
- Multiple exostoses : see relevant factsheet
Genu valgum: treatment in children
For most children with knock knees (from physiological to mild forms), it is sufficient to reassure parents and consider good personal care and active lifestyle practices (be careful not to be overweight, play sports, use appropriate footwear, etc.).
Surgical interventions: epiphysiodesis and osteotomies
For more severe cases of genu valgum , corrective surgery may be considered.
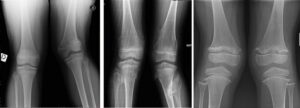
It is essential to perform a correct X-ray in preparation for possible surgery.
Hemi-epiphysiodesis (guided growth) for valgus knee: what is it and when should it be performed?
It is a minimally invasive and very effective technique for correcting genu valgum during the growth phase.
Please refer to the dedicated sheet.

Genu valgum: corrective osteotomy
This is a very effective procedure for treating knock knees, but it is more demanding than epiphysiodesis. The bones are sectioned, reoriented, and fixed in the new position using fixation devices (K-wires, plates, screws, etc.). Various options exist. Generally, immobilization is required and weight-bearing should be avoided on the operated limb initially until the bone has healed. The procedure is performed on one limb at a time. In some cases, blood transfusions are necessary.

OrthoChildren (Bologna, Italy) performs all these procedures