
Genu varum in children: physiological, idiopathic and secondary
Genu varum is defined as an alteration of the frontal axis of the lower limb that gives it a curved or “parenthetical” appearance (characterized by an increase in the space that separates one knee from the other, unlike genu valgum, which has an “X” appearance). Genu varum can affect only one limb or both.
From a technical point of view, the mechanical axis of the lower limb (the line that connects the center of the hip to the center of the ankle), in normal situations passes through the center of the knee, distributing the load symmetrically. In the case of genu varum , the axis falls more internally; in this way, the joint undergoes, both in an upright position and during walking, non-physiological stress, both on the articular cartilage and on the ligaments.
Physiological varus knee
The development of the lower limbs of children naturally passes through a phase of varus (physiological varus knee of the child). From the beginning of walking, until about 18 months of age, most children show a more or less accentuated varus that is considered physiological. This varus tends to spontaneously evolve towards a second phase of valgus (so-called “Knock-knees”). This second phase is also usually transitory: the deviation can be more or less accentuated, reaches the peak of valgus around 3.5-4 years, then the axis spontaneously returns towards the neutral axis, reaching around the age of 7-8 years the typical axis of adulthood (physiological valgus).

Idiopathic and secondary genu varum
This phase of physiological varum is often a cause of concern for families, and doctors must be able to distinguish physiological cases for which evolutionary control is sufficient without taking measures, from cases that may instead hide other problems for which earlier management is indicated.

The same applies to older children, in whom varus should no longer be present. In these cases, the pediatric orthopedist must distinguish between an idiopathic varus knee (i.e. constitutional, often on a familial basis and without underlying pathologies) and a secondary varus knee , in which there is an underlying basic pathology that causes the deviation.
Among the possible causes of secondary genu varum we can find different conditions, for example: deficiency rickets, vitamin D-resistant rickets, rickets due to renal disease, skeletal dysplasias (achondroplasia, hypochondroplasia, pseudochondroplasia, etc.), multiple exostosis disease, osteogenesis imperfecta, outcomes of infection or trauma to the growth plate, in addition to Blount’s disease (which is discussed later).
Genu varum: treatment
In idiopathic genu varum , treatment can range from simple observation, to the suggestion of adequate hygiene rules (weight control, etc.), to possible vitamin supplementation under the supervision of the pediatrician, to the use of orthoses/orthopedic shoes (now limited to very few and selected cases), up to surgery. Surgery for genu varum can range from less invasive interventions, such as asymmetric epiphysiodesis with “figure-of-8 plates”, in the case of children with active growth plates, to more invasive interventions, such as corrective osteotomies in patients who are generally at the end of their growth.
In secondary genu varum , in addition to the axis defect, the underlying pathology must be taken into consideration (which in some cases can and must be treated, for example in deficiency rickets), which is often associated with greater difficulty in treatment and a tendency to recur.
Blount’s Disease: What is it?
Blount’s disease is a growth disorder of the inner part (called medial) of the growth plate of the upper part of the tibia (called proximal tibia), which causes a progressive appearance of varus knee .
Due to the disorder, the inner part of the growth plate slows down its activity, while the outer part continues to grow. This leads to a gradual varus deformity of the knee with severe deformation of the joint structures of the knee itself.
There are two forms, based on the age of onset: the most frequent is the infantile form with onset before 8-9 years of age (usually around 2-3 years of age), however there is also an adolescent form that makes its onset after 9-10 years of age.

The typical history of the infantile form of Blount type genu varum is that of a worsening varus deformity, which progresses rapidly during the second/third/fourth year of life.
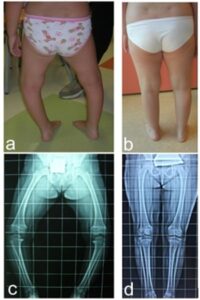
The axis of the lower limbs of affected patients (it can be just one or both) presents genu varum with a clear deviation of the leg immediately below the knee, associated with torsion of the tibia due to which the tip of the foot deviates inwards. When walking, a sort of yielding of the knee itself towards the outside can be observed (and genu varum becomes even more accentuated).
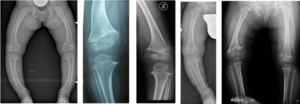
It is the task of the pediatric orthopedic surgeon to suspect Blount’s disease, distinguishing it on the one hand from the forms of physiological genu varum , and on the other from other forms of secondary genu varum . To this end, radiographic examinations may be performed to search for the typical aspects of the pathology.
Once the diagnosis of Blount’s disease has been made with certainty, treatment must be promptly undertaken.
Blount’s Disease: Treatment
Surgical treatment of Blount’s genu varum is a complex and experienced treatment.
Go to the page dedicated to the treatment of Blount’s disease
Temporary asymmetric epiphysiodesis procedure
As already mentioned, epiphysiodesis is a surgical procedure also indicated for the treatment of bow legs , which aims to stop or slow down the growth of a certain growth cartilage.
Growth plates (also called physes) are the typical structures of children’s bones that allow the various bone segments to grow in length. They can be represented as cartilage discs located at both ends of a long bone, in which the cartilage cells reproduce longitudinally and progressively ossify, thus increasing the length of the segment.
These cartilages are active throughout the child’s growth and end their activity with skeletal maturity, when the cartilage closes and is completely replaced by bone.

In the case of asymmetric epiphysiodesis: the physis is slowed down only on one side, while the remaining part of the cartilage continues to grow normally. This causes a growth deviation effect, the direction of which will depend on the point at which growth has been slowed down (if the internal part is slowed down, only external growth will continue, and vice versa).
The most commonly used synthesis device is the so-called guided growth plate: there are various models that all have the same figure-8 shape. In varus knee , these plates are positioned over the lateral growth cartilage and fixed to the bone using two screws. The surgical incision is limited to 3/4 cm. In the post-operative period, immobilization is not foreseen; from the first day, gradual mobilization of the knee and the start of loading is permitted as tolerated.
If correctly applied, the plates gradually diverge and determine the correction of the axis, with a speed proportional to the growth of the operated limb.

This is a procedure capable of significantly modifying the growth of the limbs, which can give remarkable results in the face of low invasiveness. Clearly in patients at the end of growth, there is no possibility of performing this intervention, and the only alternative to correcting the varus knee remains osteotomy. This is why it is essential that patients are promptly referred to the pediatric orthopedist, in time to carry out the appropriate assessments.
The procedure described is temporary epiphysiodesis: once the desired goal (the correct axis) has been achieved, the plates can be removed to restart cartilage growth. It is therefore a theoretically reversible procedure.
There are, however, two risks to consider:
- the risk of lesions of the growth cartilage produced at the time of the surgery and by the plate itself: once the plates have been removed, if there is still growth of the cartilage on the opposite side, the knee may continue to deviate in the direction of the correction, leading to an overcorrection (valgus knee)
- the “rebound” effect: once the plates are removed, the area of cartilage that had been slowed down starts to grow excessively again, leading to a recurrence of the varum knee
For this reason, it is necessary to perform the procedures with the correct technique and it is often preferable (when possible) to perform the surgery towards the end of growth, in order to obtain the correction of the axis and not have further growth that risks causing hypercorrection or recurrence.
In cases where the varus knee is very marked and the patient is still small, as in cases of skeletal dysplasia, it is preferable to intervene during full growth, remove the plates once the axis has been corrected, and check the behavior during the residual growth. It will be possible to repeat the procedure if the condition itself recurs.
The basis of everything is a correct preoperative evaluation.
Before the treatment of varus knee with epiphysiodesis, the clinical and radiographic aspects must be taken into consideration. It has been demonstrated that relying only on clinical measurement, neglecting the radiographic aspect, carries a high risk of making unnecessary corrections. The indication must also be limited to cases in which the alteration of the mechanical axis is significant.
Another fundamental aspect is to calculate the timing of the procedure as precisely as possible. Among the parameters that are generally analyzed we remember:
- height growth rate: patients are asked to bring all the latest height measurements taken to the visit
- pubertal development: possibly through auxological evaluation
- bone age using, as appropriate, carpal, elbow and pelvic parameters
In our experience, calculations made roughly (for example, only evaluating whether the knee cartilages are more or less open) or without taking the above aspects into consideration (for example, based only on chronological age) often lead to missed corrections.
The last fundamental aspect is the post-operative follow-up .
A program of medical check-ups is established, initially to verify that the recovery of the knee function is regular, then to verify the effect of the surgery.
To monitor the evolution of the correction, the check-ups use, in addition to clinical measurements, radiographic examinations, both of the knee (to verify that the synthesis devices are positioned correctly) and panoramic (see above) to verify the evolution of the mechanical axis.
Overall, as repeatedly emphasized, it is a non-invasive procedure for the patient and with excellent results.