
What is Perthes disease?
Perthes disease ( or Legg-Calvé-Perthes disease) is a condition in which an ischemic event affects the blood supply to the growing femoral head (epiphysis), causing ” avascular necrosis .” In simpler terms, blood flow to the femoral head is inadequate, causing bone cells to die.
Following this event, a rather typical scenario occurs in which the femoral head initially slows its development, thickens, and tends to become compressed and fragmented, and subsequently progressively restructures and remodels itself to a more or less satisfactory degree.

Perthes disease: the causes
The causes are unknown, although various factors have been implicated (alterations in coagulation, vascular microtrauma, primary anomalies in the ossification of the epiphysis, etc.).
The process affects males much more frequently (male:female ratio = 4:1) and generally on only one side (approximately 85% of cases). It is not a hereditary disease: a positive family history is very rare (5%). Perthes’ disease can manifest itself in a very wide age range ( between 2 and 13 years ) but typically strikes children between 4 and 8 years old.
Perthes’ disease: symptoms
The clinical picture initially manifests with the onset of limping in the child, who generally complains of pain in the groin, thigh, or knee .
This is a very important aspect, and it is essential to understand that in a child complaining of knee pain, it is always important to consider the possibility that the pain originates in the hip. The pain has mechanical
characteristics , meaning it resolves with rest and increases with activity. There is no fever or general malaise. Blood tests are normal. A thorough examination reveals the presence of limited movement in the affected hip (especially reduced abduction and rotation).
Perthes disease: diagnosis
Perthes’ disease is a differential diagnosis with other conditions that more frequently affect the hip in children of the same age group, primarily transient hip synovitis and osteoarticular infections . After the initial examination, blood tests, an ultrasound, and finally an X-ray will guide the doctor toward the correct diagnosis.
It is important to emphasize that while it is important not to routinely perform X-rays on every patient with limping (to limit children’s exposure to ionizing radiation), it will be necessary in all cases where joint stiffness does not resolve after a few days (as generally occurs with transient synovitis) or in cases where the diagnosis remains unclear (to exclude other possible diagnoses).
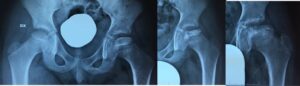
An axillary X-ray of the pelvis and hip generally allows a diagnosis of Perthes’ disease to be made in the advanced stages.
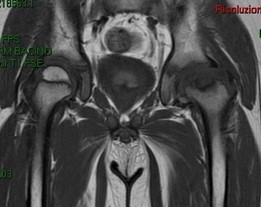
In the early stages , X-rays may not yet show signs of the disease , even though necrosis is present. In these cases, it is possible to resort to magnetic resonance imaging, for example, which can reveal the process earlier than an X-ray.
Perthes disease: the typical evolution
The pathological process involves a typical evolution of the radiographic appearance of the femur, which goes through several phases:
- Condensation phase: the femoral nucleus appears denser, “metallized”
- Fragmentation phase: the nucleus appears fragmented, “striped”, due to reabsorption of the necrotic trabeculae
- Reconstruction phase: the core is progressively restructured
- Residual deformity phase. The proximal femur gradually reaches its final shape.
Every effort should be made in managing patients with Perthes’ disease to ensure that the final shape of the femoral head is as spherical and congruent as possible with the acetabulum .
If the resulting shape is ovoid, pointed, or incongruent, or if there are macroscopic alterations to the femoral neck (coxa magna, coxa plana, coxa brevis), progressively more serious joint changes will result, resulting in premature cartilage wear (arthrosis).
Perthes disease: risk factors for prognosis
The prognosis is mainly linked to:
- Clinical signs of risk: obesity, adduction contracture, etc.
- Radiographic risk signs: Gage’s sign, metaphysitis, tendency to subluxation, lateral calcifications, etc.
- Severity of involvement. This is assessed according to the Herring (or lateral pillar) classification, which divides the lesions into groups of increasing severity (A, B, B/C borderline, C) and progressively worsening prognosis, depending on the involvement of the lateral aspect of the epiphysis.
It is important to underline that the severity of Perthes’ disease according to the Herring classification can only be assigned in the fragmentation phase , therefore in cases diagnosed early (for example in the pre-radiographic phase and in the consolidation phase) it is not possible to establish it at the first evaluation.
Conservative treatment: the goals. What is “containment”?
Let’s distinguish objectives:
- Short term: Maintain as much joint movement as possible.
- Medium term: maintain centering of the femoral head in the acetabulum.
- Long term: maintain the sphericity of the femoral head at the end of growth.
Containment is the basic principle of treatment for patients with Perthes disease : by keeping the femoral head in the acetabulum, the acetabulum acts as a cast to keep the femoral head spherical . The femoral head tends to subluxate ( progressively slide out laterally) and, in the most severe cases, develops a step-like deformity of its lateral portion (hinge abduction), which prevents the head from fully retracting into the acetabulum. To avoid or limit these consequences, orthopedists use conservative and surgical methods.
Perthes’ disease: surgical treatment
To keep the femoral head centered in the acetabulum, the orthopedic surgeon will need to evaluate the best surgical procedure ( femoral or pelvic osteotomy ) to achieve optimal femoral centering. Each procedure has advantages and disadvantages, which the orthopedic surgeon should be familiar with and discuss with the family.


Perthes disease: is an osteotomy always necessary?
No. The orthopedic surgeon will take into account the various aspects of Perthes’ disease (age, severity, risk factors, stage, etc.) to decide on the type of treatment.
For most cases of Perthes’ disease, no treatment is necessary or conservative treatment is sufficient.

In some cases of Perthes’ disease, a minor procedure to lengthen the contracted muscles or a dynamic arthrography (i.e., the injection of contrast medium into the joint) will be considered to better assess whether the femoral head has the ability to center itself or not.
Wouldn’t it be better to wait as long as possible and then possibly perform the operation?
Unfortunately, this is incorrect reasoning. Surgery for Perthes’ disease should be considered in the initial stages of fragmentation, therefore rather early. One of the most common mistakes is deciding to operate too late , when the femoral head has already deformed, with very poor results.

OrthoChildren Center is an experienced center for Perthes disease