
Tarsal coalition: clinical presentation
Tarsal coalitions are malformations in which the tarsal bones (i.e. the back of the foot: talus, calcaneus, navicular, cuneiform, cuboid), instead of being separated from each other, have one or more connections that limit or block their movement.
This is a relatively rare problem (reported, depending on the case studies, between 0.03 and 1% of the healthy population) but it must be kept in mind when evaluating and treating children’s feet.
Tarsal coalitions: causes
The cause of this anomaly is unknown. Physiological fetal development involves a progressive segmentation of the tarsal cartilages; in cases of coalition, this separation is incomplete for an unknown reason. In some rare cases, there is a family history.
In 50-60% of cases, the condition is bilateral.
Tarsal coalitions: types and presentation
The most frequent types of tarsal coalitions are that between the talus and the calcaneus and that between the calcaneus and the scaphoid , but other types of coalitions are possible, sometimes even simultaneously.
Although coalitions are generally present from birth, symptoms appear at a later age , as the cartilaginous structures ossify and the functional demands (and weight) of the patient increase: typically patients become symptomatic between the ages of 12 and 15 years in the case of talo-calcaneal coalitions and a little earlier (between 9 and 12 years) in the case of calcaneo-scaphoid coalitions.
The presence of coalition causes abnormal overloading of the foot joints, which creates pain and painful spasm of the muscles. The pain is mostly referred laterally (sinus tarsi) or medially (under the medial malleolus) or along the arch of the foot, especially during activities that involve walking or running on uneven surfaces (due to the reduced mobility of the subtalar joint). Repeated sprains are often reported, precisely because of the foot’s poor ability to adapt to changes in terrain.
Furthermore, the foot may show a deformity: flatfoot, valgus foot and abduction of the forefoot.
When to suspect tarsal coalitions?
Patients with tarsal coalition may present with a painful flatfoot or valgus foot : in this case we speak of a “rigid” flat foot.
It’s crucial for clinicians to distinguish these (rarer) situations from the more common “flexible” flatfoot conditions. For example, the use of traditional corrective surgical procedures for flexible flatfoot (calcaneo stop, etc., see fact sheet) isn’t as effective for rigid flatfoot and can actually worsen the stiffness if the coalition isn’t recognized and treated appropriately.
The main characteristic of rigid flatfoot due to coalition is reduced mobility of the subtalar joint. This is clinically evident with both passive and active maneuvers. Passively, when moving the hindfoot, limited inversion and eversion are observed; in some cases, actual foot contracture (“contracted foot”) is present due to painful spasm of the peroneal muscles, which impede inversion movements of the foot and further pronate it. Actively, if the patient is asked to stand on tiptoe, the physiological heel inversion observed in flexible flatfoot is not observed.
In these cases it is advisable to request further diagnostic testing.
What investigations should be requested in case of suspected tarsal coalitions?
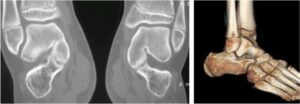
The presence of tarsal coalition can be suspected even from a simple radiographic examination based on some indirect signs (for example, the presence of an osteophyte on the talar neck). If coalition is clinically suspected, as a first approach, it may be useful to request, along with two weight-bearing X-rays of the foot, an oblique view of the foot, which can easily demonstrate a coalition between the calcaneus and the navicular (but does not allow for the detection of other types of coalition).

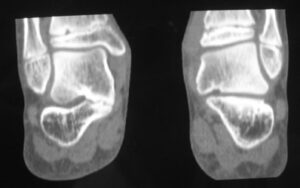
The best test for studying coalitions is undoubtedly CT, which allows us to highlight their location, type (some fusions are complete, others are incomplete or fibrous) and extent (sometimes these are limited fusions, sometimes very extensive blocks in which it is difficult to imagine a restoration of motility).
MRI also has a role and can be considered as an initial approach to limit radiation exposure associated with performing CT.

Treatment of tarsal coalition
In case of pain, a non-surgical treatment attempt using orthoses, physiotherapy or immobilization may be indicated depending on the clinical picture present.
If this approach fails, surgical treatment is indicated , which typically includes:
- resection of the synostosis
- the interposition of tissue to avoid the risk of new ossification of the synostosis
- possibly the correction of associated valgus foot or flatfoot (arthroereisis, calcaneo stop, osteotomies, etc.: see fact sheet)
Calcaneoscaphoid coalition: treatment
It is treated through a dorsolateral approach; once the edges of the coalition have been identified, it is resected, taking care not to damage the adjacent joints, to avoid leaving plantar fusion bridges, and to avoid excessive resection. For interposition, the pedis muscle can be used, or alternatively, local adipose tissue or bone wax.
Endoscopic resection is a minimally invasive surgical option for treating tarsal coalition
Talocalcaneal coalition: treatment
Resection of these coalitions is more complex than that of calcaneonavicular coalitions. The coalition is treated through a medial approach, working deep to the posterior tibial sheath and the digital flexor sheaths. The fusion is often not directly visualized and must be identified indirectly by searching for the “free” joint anterior and posterior to the synostosis itself.

Interposition can be performed by applying bone wax, local adipose tissue, or bone bank tissue (e.g., fascia lata).
Endoscopic resection is a minimally invasive surgical option for treating tarsal coalition
In case of very extensive colition or in case of failure to resolve symptoms after resection of the synostosis, a subtalar arthrodesis is indicated.
The results of surgery for tarsal coalitions
Long-term results of tarsal coalition resection are generally good. Failures may be related to incomplete resection or the treatment of very extensive coalitions, i.e., those involving a large portion of the subtalar joint.
Gait analysis studies have, however, highlighted how even in patients who show improvement in passive subtalar motility and resolution of the disorders, a limitation of inversion-eversion movements during walking or running and an incomplete normalization of plantar pressures during walking may remain.
In essence, surgery can restore mobility at this level and resolve the symptoms, but it is not possible to completely normalize a foot that has developed with a more or less extensive malformation, and the family must be informed of this.
Essential bibliography
- Kothari A, Masquijo J. Surgical treatment of tarsal coalitions in children and adolescents.EFORT Open Rev. 2020 Feb 26;5(2):80-89.
- Docquier PL, Maldaque P, Bouchard M. Tarsal coalition in pediatric patients. Orthop Traumatol Surg Res. 2019 Feb;105(1S):S123-S131
- Guignand D, Journeau P, Mainard-Simard L, et al: Child calcaneonavicular coalitions: MRI diagnostic value in a 19-case series, Orthop Traumatol Surg Res97:67, 2011
- Hetsroni I, Ayalon M, Mann G, et al: Walking and running plantar pressure analysis before and after resection of tarsal coalition, Foot Ankle Int28:575, 2007.
- Hetsroni I, Nyska M, Mann G, et al: Subtalar kinematics following resection of tarsal coalition, Foot Ankle Int29:1088, 2008.
- Mubarak SJ, Patel PN, Upasani VV, et al: Calcaneonavicular coalition: treatment by excision and fat graft, J Pediatr Orthop 29:418, 2009
Patients from abroad: can OrthoChildren Center treat foreign patients?
Yes, many patients come from all countries (Europe and USA):
- the surgical equipe has a wide experience with Tarsal coalitions
- an intensive rehabilitation program can be included
- the procedure is less expensive than in USA and other countries
- Families take advantage of this opportunity to combine a trip to the beauties of Italy