
Sprengel’s deformity (congenital high scapula) is a deformity in which the scapula is positioned higher than normal. It can cause aesthetic or functional changes that are more or less disabling. Treatment requires a center with specific experience, like OrthoChildren Center.
What is Sprengel’s deformity: congenital high scapula?
Sprengel’s deformity is a deformity in which the scapula is positioned higher than normal. This congenital anomaly, depending on the severity of the condition, can cause purely aesthetic or functional changes that are more or less disabling.

Sprengel’s deformity: causes
The causes responsible for Sprengel’s deformity are not fully understood.
We know that during the physiological development of the fetus, the scapula forms as an appendage at the level of the cervical vertebrae. Gradually, within the first three months of fetal life, it descends posteriorly until reaching its final position in the upper part of the thoracic wall.
The genesis of congenital high scapula is based on a more or less precocious anomaly in this developmental or descent process. These alterations can also lead to complex pathological conditions, in which not only the height of the scapula is altered but other surrounding structures may also be affected. It is not uncommon for high scapula to be associated with malformations, retractions, or fibrosis of the muscles surrounding the scapula; malformations of the cervical vertebrae (e.g., Klippel-Feil syndrome); altered shape or orientation of the scapula itself (e.g., its uppermost portion may be deformed, assuming a concavity that follows the upper part of the chest wall, a so-called “pagoda” deformity), etc.
In approximately one third of cases of congenital high scapula , the so-called “homovertebral bone” is present: a bony bar that connects the scapula to the vertebrae, preventing their migration and normal movements.

Sprengel’s deformity: manifestations
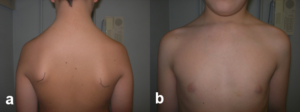
The clinical appearance is highly variable. There are mild cases of high scapula , in which the only finding is a modest asymmetry of the shoulder girdle and neck profile, in the absence of functional disorders. These cases are often not evident at birth but rather during growth and must be differentiated from cases of scoliosis, which may present with apparently similar characteristics. Surgical treatment is not necessary.
In more severe cases, the diagnosis is made at birth or in the first few years of life. In these cases, the condition progresses with growth, primarily as a result of the altered developmental dynamics of the muscles surrounding the scapula.

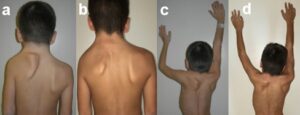
Congenital high scapula can be unilateral or bilateral, and as mentioned, its severity can vary. The high scapula can be 1 to 12 cm higher than the scapula on the unaffected side. When very raised, it gives the neck a broad, squat appearance, a feature that becomes even more pronounced when associated with vertebral malformations typical of Klippel-Feil disease.
From a functional point of view, shoulder abduction movement (i.e. the movement of the arm away from the trunk) is limited to a greater or lesser extent and some children are unable to move beyond the shoulder line, resulting in serious functional limitations in daily life.

The diagnosis of high scapula must be differentiated from other conditions that may appear similar to the untrained eye, such as “winged” (alata) scapula, scoliosis, scapular exostoses, obstetric palsies, etc. It is also important not to limit the examination to the scapula alone, but to exclude possible associated problems, such as Klippel-Feil syndrome, spinal cord abnormalities, and possible associated syndromes. The required diagnostic tests generally include X-rays, CT scans, and MRIs.

Treatment of Sprengel’s deformity (congenital high scapula)
In the mildest cases of high scapula , in which there is no functional disorder and the aesthetic defect is minimal, no specific treatment is indicated, while physical activity that includes muscle strengthening and stretching of the shoulder girdle is recommended.
In severe cases of congenital high scapula, however, treatment becomes more complex. While a re-education program aimed at regaining as much movement and muscle strength as possible may be indicated in younger children, surgery should be considered as the patient grows, and in the presence of an aesthetically unacceptable deformity or obvious functional limitation.
The age at which corrective surgery for high scapula is generally recommended is between 3 and 7 years: before this age the procedure can be technically more difficult, while beyond this age there is a greater risk of complications.
However, the pediatric orthopedic surgeon will evaluate each individual case to decide the optimal age and type of procedure. For example, when there is complete blockage of scapular motion due to the presence of a complete omovertebral bone, the benefits of postponing surgery for rehabilitation will be limited.
Sprengel’s deformity: surgical procedures
There are several surgical techniques for treating high scapula. The most commonly used are the modified Green technique, the modified Woodward technique, and techniques involving a scapular osteotomy (Mears, etc.).
These techniques involve multiple surgical procedures aimed at correcting the various aspects of the deformity. The muscles connecting the upper scapula to the vertebrae, the chest wall, and the humerus are progressively detached. The scapula is freed from all adhesions to surrounding structures, and, if present, the omovertebral bone is removed.
In the most severe cases of congenital high scapula , when a bone deformity is present, it may be necessary to remove the upper end of the bone itself. Some techniques may involve an osteotomy of the scapula, which involves splitting the bone into two parts.
Once freed (and possibly straightened), the scapula is then translated to a lower position, as far as the tension of the surrounding structures and the severity of the situation allow. However, it is often not possible to achieve symmetry with the unaffected side, both due to the risk of excessive tension on the vascular and nervous structures and the size and shape of the affected scapula, which ultimately represent a factor of asymmetry.
Finally, the scapula is fixed in the desired position in different ways (creating a pocket under the latissimus dorsi muscle, fixing it to the ribs, etc.) and the muscles that were initially detached are reinserted in the new position.
Once the suturing is complete, the limb is immobilized with a bandage, which usually lasts for about 3-5 weeks. Once the bandage is removed, the motor rehabilitation program begins.
Results of surgical treatment of Sprengel’s deformity
The results of surgical treatment of congenital high scapula are generally very good, both functionally (improved shoulder motion) and aesthetically. However, the procedure is fraught with a certain risk of complications, which can be minor (hypertrophic scarring, winged scapula, insufficient lowering, etc.) or major (pneumothorax, vascular-nervous deficits, etc.).
The main risk is the appearance, after the procedure, of vascular and/or nervous disorders in the operated limb, due to the excessive tension created by the lowering of the scapula. In these cases, it becomes necessary to re-operate on the patient to reduce the tension (by reducing the achieved lowering or by performing a clavicle osteotomy; some authors recommend performing this osteotomy first in more severe cases of high scapula).
Timing is crucial to achieving good results. It is therefore crucial that the patient receives early follow-up by a physician experienced in treating this deformity. Precise surgical planning, careful monitoring for potential complications, and a proper rehabilitation program are certainly the foundation for best results in the treatment of congenital high scapula.
OrthoChildren Center has a long experience with these procedures.
Patients from abroad: can OrthoChildren Center treat foreign patients?
Yes, many patients come from all countries (Europe and USA):
- the surgical equipe has a wide experience with Sprengel’s deformity
- an intensive rehabilitation program can be included
- the procedure is less expensive than in USA and other countries
- Families take advantage of this opportunity to combine a trip to the beauties of Italy