
Slipped capital femoral epiphysis is a pediatric orthopedic pathology that mainly affects adolescents, characterized by a slippage of the femoral head with respect to the femoral neck.

This pathology can affect the femur on one side only (unilateral) or both femurs (bilateral) simultaneously or at different times.
Males are more affected than females (recent studies show a male-to-female ratio of approximately 2:1) with a peak in the disease in adolescence (average age 13.4 years in males and 12.2 years in females).
Slipped capital femoral epiphysis: causes
Slipped capital femoral epiphysis is caused by an area of weakness at the proximal physis of the femur where excessive forces cause the proximal metaphysis of the femur to “slip” relative to the epiphysis.
In the early stages, this pathology is characterised by a pre-slip condition, with areas of alteration of the physis, identifiable by magnetic resonance imaging.
Various risk factors can favor its onset.
From a mechanical point of view, a higher incidence has been demonstrated in subjects who present an alteration of the perichondrial ring at the level of the physis, an increased retroversion of the femoral neck and finally an increased inclination of the physis with respect to the femoral neck.
Furthermore, several studies report close correlations with obesity ; in these cases, the presentation is more frequently early and bilateral.
Other risk factors that may predispose to slipped capital femoral epiphysis include endocrine conditions . Indeed, children with hypothyroidism, renal osteodystrophy, panhypopituitarism, and growth hormone deficiency may have a higher incidence.
Slipped capital femoral epiphysis: clinical forms
There are various ways to classify this pathology.
From a temporal point of view, slipped capital femoral epiphysis can be classified according to the onset of symptoms.
- Acute: When symptoms have been present for less than 3 weeks, the patient experiences severe pain and is unable to walk. X-rays typically show a slippage with a distinct step between the metaphysis and epiphysis.

- Chronic when symptoms have been present for more than three weeks, the patient often presents with vague pain for months, along with limping. X-rays typically show bone remodeling.

- Acute on chronic when vague symptoms that have been present for many months suddenly develop into a sharp, persistent pain that prevents walking. Radiographically, both slippage and bone remodeling are evident.
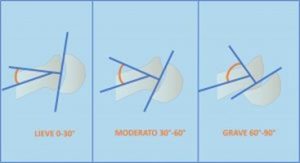
Another classification of slipped capital femoral epiphysis is based on morphology and the degree of slippage: mild, moderate, or severe. Different methods are used to calculate this “slippage.” Southwick recommends using the head-shaft angle in posterior (AP) and lateral (Frog-Leg) pelvic X-rays. This angle is considered mild when it is less than 30°, moderate when it is between 30° and 60°, and severe when it is greater than 60°.
Finally, from a clinical point of view and for the purposes of therapeutic choice, the functional classification based on the patient’s ability to walk is fundamental.
- Stable epiphysis when the patient is able to support himself with full or partial weight bearing with or without the use of crutches.
- Unstable epiphysis when the affected lower limb is unable to bear weight.
Slipped capital femoral epiphysis: symptoms
The patient affected by slipped capital femoral epiphysis presents symptoms directly proportional to the severity of the clinical picture.
Stable and chronic conditions are characterized by pain in the anteromedial region of the thigh, sometimes also referred to the knee.
Unfortunately, it’s common for pain to be localized exclusively to the knee (and not the hip) and has led to delayed diagnoses. These patients often undergo diagnostic tests and treatments aimed solely at the site of the pain. However, it’s a fundamental principle in pediatric orthopedics that all children presenting with knee pain should also be evaluated (at least clinically) at the hip on the same side. And the suspicion for a slipped capital femoral epiphysis should be heightened the more the patient is at risk and has typical physical characteristics.
The painful symptoms have mechanical characteristics (i.e. they are not present at rest, but increase under load and with activity).
The physical examination reveals pain during hip rotation (especially during internal rotation), forced external rotation during hip flexion (Drehmann’s sign), and possible shortening and external rotation of the limb in more advanced cases.
In acute and acute-on-chronic cases, the child will present with an incomplete ability to walk. Severe pain will be present, and the limb will be positioned in flexion and external rotation to try to relieve the pain.
Slipped capital femoral epiphysis: radiographic diagnosis
If a slipped capital femoral epiphysis is suspected , it is essential to request anteroposterior (AP) and frog-leg (Danlop or Lauenstein) pelvic x-rays. Only if there is a strong suspicion of hip unstable hip (in which the clinical presentation sometimes resembles a proximal femoral fracture) is it advisable to avoid frog-leg x-rays and decide whether to perform one only after evaluating the AP projection.
In the presence of manifest epiphysiolysis, slippage between the epiphysis of the proximal femur and the metaphysis will be immediately evident.
However, if the disease is in an initial stage, some radiographic signs will allow us to identify the actual “slippage” early.

In case of mild initial slippage, we use the Klein line: in a normal hip (right hip) this intersects the most lateral part of the femoral head, while in a pathological hip (left hip) this does not happen.
X-rays will also allow us to measure the severity of the slip and to distinguish between chronic, acute, and acute-on-chronic conditions.
Magnetic resonance imaging is indicated both in suspected cases and in cases where one wishes to more precisely evaluate the direction and extent of the slip.
In fact, in the pre-slipping phase, only a widened and irregular physis may be evident. If there is strong clinical suspicion, an MRI scan is recommended, which will reveal an area of edema right at the level of the physis.
Slipped capital femoral epiphysis: treatment
Treatment for slipped capital femoral epiphysis is always relatively rapid and surgical , with the primary goal of preventing further slippage of the femoral head. The earlier treatment is performed, the more minor procedures will be sufficient and the prognosis will be better. Greater slippage exposes the hip to a worse prognosis (higher risk of necrosis, early osteoarthritis, and the need for complex procedures).
The main distinction must be made between cases with stable presentation (the most frequent) in which surgery must be performed relatively quickly, and those with acute presentation (rarer) in which treatment is instead to be considered a true emergency.
As previously explained, in this second case, the femoral head suddenly slips relative to the femoral neck, which can cause damage to the vessels supplying blood to the femoral head. A significant delay in reducing the slippage can increase the risk of femoral head necrosis.
In both cases, if diagnosis and treatment are performed in the pre-slip or mild slippage phase, the gold standard treatment is so-called “in situ fixation.” This involves inserting a screw that blocks the slippage between the femoral head and neck, thus preventing the condition from worsening.

Percutaneous techniques are generally used (i.e., minimally invasive, without the need for large incisions). Postoperatively, the patient will begin walking with the aid of two crutches and initially with a protected weight, subsequently gradually increasing the weight.
In cases of severe slippage, it is necessary to evaluate the possibility of performing more complex surgical procedures, such as triplanar osteotomies, surgical dislocation of the femoral head with reshaping of the femoral neck, etc., in order to best restore the joint’s relationship. These are more complicated procedures (described beyond the scope of this factsheet) and present additional risks, including necrosis of the femoral head.
All the more reason to underline the importance of a timely diagnosis of slipped capital femoral epiphysis and early treatment, precisely to avoid reaching severe pathological conditions and having to resort to major procedures, and to limit the risk of complications.
Slipped capital femoral epiphysis: what to do on the unaffected side?
This represents another important point. In fact, while in cases involving both femurs simultaneously, there is no doubt that both hips should be operated on, in cases where only one femur is affected by slipped capital femur , there is a risk that in the following months or years, the unaffected hip will also slip.
For this reason, the orthopedist will need to decide whether to prophylactically fix this hip (even if it’s not affected) or monitor it over time. Both decisions have risks and benefits: on the one hand, the risk of iatrogenic injury to a healthy hip if the fixation is performed; on the other, the risk of the initially healthy hip slipping severely later if it’s not fixed.
To support this decision, some clinical and radiographic elements are used (for example, the Oxford Hip Score) which indicate an increased risk in certain situations (age less than 10 years, obesity, open triradiate cartilages, associated endocrinopathies) for which preventive contralateral fixation will more frequently be recommended .
Even in this case, however, it is important to consider the correct fixation technique: if you decide to fix the unaffected hip, it is essential to use surgical techniques that allow the femoral neck to continue growing, if the residual growth is significant.
Why is it important to consult an experienced pediatric orthopedic surgeon?
Slipped capital femoral epiphysis is one of the conditions most frequently diagnosed late (even after months of limping), thus preventing early and simple treatment.
It is advisable to always maintain a high level of suspicion for this condition (especially in cases with a typical presentation), perform the required tests early (X-rays and possibly MRI) and promptly consult an experienced pediatric orthopedist.
The prognosis (i.e. the functioning of the affected hip) will in fact be very good in case of adequate and early treatment, while it risks being severe in case of inadequate treatment or in a very advanced stage.