Posteromedial Bowing of the Tibia: what is it?
Posteromedial Bowing of the Tibia (ot Congenital tibia recurvata) is a rare congenital condition that manifests at birth with a deformity of the lower leg bones, resulting in recurvation and valgus.
In other words, the tibia and fibula present a curvature, usually at the transition between the middle and lower third of the shaft, with the apex of which is posterior and medial.

Cases of posteromedial bowing of the tibia are rare but the characteristics are constant and include various aspects.
Posteromedial bowing of the tibia: clinical presentation
At birth, patients very often present with a talovalgus foot. The foot appears strongly dorsalized, with its dorsum close to the anterior part of the leg, and in a valgus position. When attempting to bring the foot into a neutral position, tension in the anterior muscles is evident.
Talovalgus foot is generally quite common and easily resolved in the “healthy” population, but it is important to keep this possible association in mind and check whether the malposition of the foot is associated with a deformity of the leg.
If associated with tibia recurvata, it is advisable to proceed with conservative treatments (manipulation, splints, braces, etc.) to normalize the position of the foot.

In posteromedial bowing of the tibia, the recurvation and valgus deformity is most severe at birth and then tends to improve spontaneously on both planes . Improvement is slow and progressive and occurs in all cases.
The maximum rate of improvement occurs in the first year, but improvement generally continues until the age of 4-5 years .
In a portion of patients with tibia recurvata, this improvement leads to a total or almost total correction of the deformity.

In the remaining children with congenital tibia recurvata , a significant leg deformity remains and requires correction.

In congenital posteromedial bowing of the tibia, secondary deformities can also occur , both above (varism and procurvation of the proximal tibia) and below (deformity of the ankle, compensation of the subtalar joint, retraction of the Achilles tendon).
Posteromedial bowing of the tibia: short leg
All cases of posteromedial bowing of the tibia present with shortening of the leg, the extent of which varies considerably.
A typical feature of this condition is that only the lower leg (i.e., from the knee down) is affected , while the two femurs (thighs) are symmetrical.
Shortening in congenital tibia recurvata is mild to moderate at birth, but over time the length difference behaves like in cases of congenital LLD according to Shapiro, that is, it tends to increase linearly and proportionally over the years . This should be made clear to parents from the first visits; LLD generally does not remain constant: what remains constant is the percentage of shortening compared to the healthy leg, and therefore the length difference will tend to increase over the years. Often, in posteromedial bowing of the tibia, this length difference is greater than 3-4 cm (sometimes even 7-8 cm) and requires lengthening surgery to restore equal length between the two limbs.
Since the percentage of shortening remains constant with growth, it is possible to predict the difference in length between the two limbs at the end of growth. For example, online applications based on Professor Dror Paley’s Multiplier system allow for these calculations.
When performing these calculations, it should be kept in mind that the accuracy of the calculations may be more limited in children under 4 years of age due to the potential risk of less accurate X-rays.
Once the prognosis for length discrepancy at the end of growth has been calculated, it will be possible, right from the first visits, to establish a treatment plan for congenital tibia recurvata .
Treatment of posteromedial bowing of the tibia
In the initial stages, no specific treatments are necessary for posteromedial bowing, other than those for talovalgus foot.
Children will begin to walk without difficulty. Insoles, braces, and lifts may be useful to facilitate walking, depending on the presence of significant deformities and length discrepancies.
In the early years , progressive improvement of the deformities and the increase in leg length discrepancy should be monitored .
It is also important, at this stage, not to overdo the X-rays, to limit the child’s exposure to radiation.
Subsequent treatment for congenital tibia recurvata will then vary depending on the extent of the leg length discrepancy and whether the deformity has been corrected.
Symmetrical hemi-epiphysiodesis for posteromedial bowing
For cases of posteromedial bowing of the tibia with minor differences in length (expected at full growth) (approximately between 2 and 3/3.5 cm), it is possible to choose not to lengthen the pathological short leg, but to slow the growth of the healthy leg (see dedicated fact sheet).
This is a more limited procedure than lengthening and results in much faster functional recovery. This option should be discussed thoroughly with the family due to its risks and benefits.
Leg lengthening for posteromedial bowing
In cases of posteromedial bowing of the tibia where the deformity is corrected, but only a significant length discrepancy remains, leg lengthening with an external fixator will be performed. This procedure is usually performed at the end of growth, so that the amount of lengthening required can be precisely calculated. Alternatively, it can be performed earlier, based on the growth prediction calculations, but taking into account the potential risk of calculation errors or growth variations.
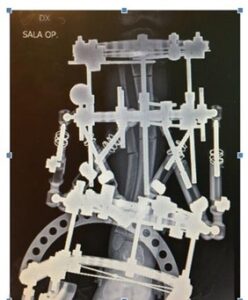
Lengthening with deformity correction or bifocal lengthening
In cases of posteromedial bowing of the tibia where a significant deformity persists, it is possible to correct it using the same procedure and simultaneously lengthen the leg. This is typically done using hexapodal external fixators with computerized software.