
Flat feet in children: what treatments are available?
There are numerous surgical procedures for correcting flat feet. Generally, the techniques are divided into:
- Arthroereisis (calcaneo stop, endorthesis, etc.)
- Osteotomies
- Arthrodesis (joint fusions)
While osteotomies and arthrodesis are typical for flat feet at the end of growth, arthroereisis is best used in growing children.
Joint preservation remains the priority, so arthrodesis should be reserved for extreme cases and generally not for flexible flat feet in children and adolescents without underlying pathologies.
Calcaneal osteotomy procedures, often combined with soft tissue procedures, are more demanding than arthroereisis procedures (one side is operated on at a time, requiring prolonged immobilization), but multiple studies have demonstrated excellent short- and long-term results when performed with the right indications.
Arthroereisis (calcaneo stop, endorthesis, etc.) for the correction of flat feet
Arthroereisis surgery (calcaneo stop, etc.) for flat feet is a relatively simple procedure. There are several variations, but they all share some common characteristics. To put it simply:
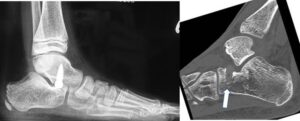
- it involves applying an implant (screw, spacer, etc.) from a lateral access (just below and anterior to the lateral malleolus) at the level of the sinus tarsi
- The screw or implant modifies the relationship between the two bones that make up the back of the foot (the talus and the calcaneus). The talus (which has slipped in flat feet ) is raised and a stop (hence the term calcaneal stop or calcaneal stop ) is provided to the excessive inclination of the heel. A ” proprioceptive ” effect is also hypothesized, that is, stimulation of the nerve fibers present at this level, which would, over time, stimulate the formation of the plantar arch.
- the surgical wound is very small
- functional recovery is quite rapid : generally the patient is allowed to walk immediately, with high shoes or protective braces;
- If necessary, additional surgical procedures may be associated (Achilles tendon lengthening, medial recovery, accessory scaphoid resection, etc.).
Arthroereisis, Endorthesis, and Calcaneo Stop: Where is the implant inserted?
The implant for flat foot arthrisis surgery can be inserted:
- in the sinus tarsi (endorthesis)
- screwed into the heel (calcaneus or calcaneus stop)
- screwed into the talus (calcaneus or calcaneus stop).
Generally, implants screwed into the bone present less of the risk present in endortheses, namely that the implant can be rapidly expelled to the surface.
Arthroereisis, Endorthesis and Calcaneal stop: which material?
We can distinguish:
- absorbable materials
- non-absorbable materials.
Each has its own advantages and disadvantages . For example, the absorbable implant has the advantage of not requiring removal in most cases, but it can sometimes fail prematurely and cause loss of correction or synovitis.
The non-resorbable metal implant generally has a superior mechanical strength, but often needs to be removed.
Which arthroereisis/calcaneo stop technique is superior?
The possible options for surgery for flat feet are largely based on the surgeon’s personal preference and experience, without establishing a clear distinction between indications.
Many orthopedic surgeons have switched from one type of implant to another over time, indicating that no single procedure is definitively superior to another and that surgeons themselves feel the need to optimize results that are not yet entirely satisfactory.
Arthrorisis, Endorthesis and Calcaneal Stop: At What Age?
Generally, these procedures are indicated and achieve the best results between the ages of 9 and 12.
Simply put, the procedure takes advantage of the growth of the foot, which changes its morphology as it grows; as it grows, the structures adapt to the new situation and the presence of the implant is no longer necessary; therefore, the screw can be removed or reabsorbed.
This age range therefore represents a general but not rigid rule , and should be reassessed on an individual patient basis. For example, some children exhibit premature skeletal (and foot) growth. The procedure can sometimes also be performed on older patients whose feet have remained flexible, although it is important to note that the results may be inferior , as the aforementioned adaptation of the structures with growth is not possible.
It is important to emphasize that age should not be a reason for hasty surgical decision-making . That is, just because a patient is about to turn 12 does not mean they should undergo surgery quickly and without adequately evaluating the risks, benefits, and alternatives.
Our preference
We generally use a non-absorbable metal screw inserted into the talus . For specific cases, we recommend an absorbable screw.
The results of surgeries for flat feet: scientific evidence, a critical analysis
A review of the most recent literature on pediatric flatfoot surgery offers no absolute certainty . This is because most studies include a limited number of patients, unclear indications for surgery, often including patients with conditions other than flexible flatfoot or with very different ages, a lack of standardized evaluation criteria (sometimes exclusively radiographic!), and retrospective studies or follow-up that is too short (sometimes two months!).
Arthroereisis, Endorthesis and Calcaneal Stop: Results
Despite the aforementioned limitations, most authors report (and this is our own experience) good results in terms of satisfaction, quality of life and radiographic correction, and return to sports activity in pediatric patients with symptomatic flexible flat foot .
Final considerations: a simple and effective intervention for flat feet, but with the right indications
The arthroereisis procedure (in one of its proposed methods) is a simple procedure and produces good short-term results in the majority of cases .
It is essential that the procedure be proposed with the right indications , primarily in symptomatic patients , otherwise children are exposed to a risk of complications that are difficult to justify.
In the case of symptomatic patients with the characteristics highlighted above ( flexible flat feet , preferably between 9 and 12 years old, significant pain, etc.), who have not responded to conservative treatments, arthroereisis can represent an excellent solution to the problem and allow for anatomical and functional improvement.
However, the risks associated with possible complications and failures must be considered , and these must be weighed against the actual problems and discussed with the family.
Flat foot with tarsal coalitions: can it be treated?
Yes, but both aspects must be considered: flatfoot and coalitions. Please refer to the fact sheet dedicated to tarsal coalitions.
Essential bibliography on flat feet in children
1- Uden H, Scharfbillig R, Causby R. The typically developing pediatric foot: how flat should it be? A systematic review. J Foot Ankle Res. 2017 Aug 15;10:37.
2- Banwell HA, Paris ME, Mackintosh S, Williams CM. Pediatric flexible flat foot: how are we measuring it and are we getting it right? A systematic review. J Foot Ankle Res. 2018 May 30;11:21.
3- Choi JY, Hong WH, Suh JS, Han JH, Lee DJ, Lee YJ. The long-term structural effect of orthoses for pediatric flexible flat feet: A systematic review. Foot Ankle Surg. 2020 Feb;26(2):181-188
4- Tudor A et al. Flat-footedness is not a disadvantage for athletic performance in children aged 11 to 15 years. Pediatrics 2009;123 (3): e386-92
5- Mosca V. Flexible flatfoot in children and adolescents. J Child Orthop. 2010 Apr; 4(2): 107–121.
6- Kubo H, Lipp C, Hufeland M, Ruppert M, Westhoff B, Krauspe R, Pilge H. Outcome after subtalar screw arthroereisis in children with flexible flatfoot depends on time of treatment: Midterm results of 95 cases. J Orthop Sci. 2019 Jun 26.
7- Faldini C, Mazzotti A, Panciera A, Persiani V, Pardo F, Perna F, Giannini S. Patient-perceived outcomes after subtalar arthroereisis with bioabsorbable implants for flexible flatfoot in growing age: a 4-year follow-up study. Eur J Orthop Surg Traumatol. 2018 May;28(4):707-712
8- Bernasconi A, Lintz F, Sadile F. The role of arthroereisis of the subtalar joint for flatfoot in children and adults. EFORT Open Rev. 2017 Nov 8;2(11):438-446
9- Shah NS, Needleman RL, Bokhari O, Buzas D. 2013 Subtalar arthroereisis survey: the current practice patterns of members of the AOFAS. Foot Ankle Spec 2015;8:180-185
Patients from abroad: can OrthoChildren Center treat foreign patients?
Yes, many patients come from all countries (Europe and USA):
- the surgical equipe has a wide experience with these procedures
- an intensive rehabilitation program can be included
- the procedure is less expensive than in USA and other countries
- Families take advantage of this opportunity to combine a trip to the beauties of Italy