
What is femoral anteversion?
Definition of femoral anteversion:
Femoral anteversion corresponds to the angle formed by the femoral neck relative to the femoral shaft in the coronal plane. It corresponds to how much the femoral neck points forward relative to the plane of the rest of the femur .
If instead you look at it from the reverse perspective, that is, with respect to the plane of the femoral neck (which articulates in the pelvis at the hip level), it corresponds to how much the femur looks inwards, and this helps to understand how the final effect of excessive anteversion will be the internal rotation of the limb.
Physiological development of femoral anteversion
All newborns have a high degree of femoral anteversion at birth, approximately 30-40°. Physiologically, anteversion decreases spontaneously and progressively throughout growth. This reduction occurs primarily up to the age of 10-12 years, but continues slowly until skeletal maturity, reaching the typical adult value of approximately 15°.
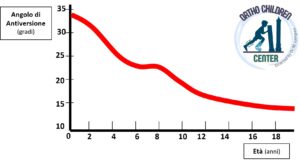
The physiological development of femoral torsion during growth is part of the harmonious development of torsions and rotations of the lower limb and helps maintain a correct angle of the child’s step.
However, this curve represents an average. Variations within the population are possible, which often lead families to worry about their child’s gait.
Clinical presentation of excessive femoral anteversion
Some children present with excessive femoral anteversion , that is, with an anteversion greater than that expected for their age.
The condition is more common in the 3 to 6 year age group (before this age, anteversion is present but is masked by the physiological external rotation contracture of the hips, typical of the first months of life), more common in females and can sometimes be found in other family members.
It is usually bilateral (if unilateral, it may indicate an underlying pathology) and is not associated with other underlying conditions. It is hypothesized that it may be favored by specific intrauterine positions (for example, in situations of excessive fetal weight or insufficient amniotic fluid, etc.).
Children present with:
- Walking with the toes turned inward; this internal rotation is usually not constant, but varies from one step to the next; children are able to control themselves on demand, but then resume walking as before.
- Sitting in the “W” position: children feel more comfortable sitting in this position (in which the femur is more centered in the pelvis) and have difficulty sitting in the Indian position.
- There is no pain
- Running appears uncoordinated
- It can sometimes lead to difficulties and falls (“ tripping over one’s own feet ”)
Clinical evaluation of femoral anteversion
Observation of gait should confirm that internal rotation occurs at the proximal level: during walking, the patellae point inwards.
The simplest way to assess femoral anteversion is to examine the patient in the prone position and assess the hip rotation arc. Excessive anteversion will result in increased internal rotation (over 60-70°) and decreased external rotation (less than 20-30°).
Another useful test is to palpate the greater trochanter throughout the arc of hip rotation and calculate the angle of internal rotation of the hip at which the greater trochanter appears most prominent.
Furthermore the examiner must:
- Differential diagnosis with respect to other possible causes of inward walking : internal tibial torsion, metatarsus varus
- Rule out underlying causes that may lead to excessive femoral anteversion: for example, neurological and neuromuscular pathologies, hip dysplasia, motor developmental delays.
Are X-rays necessary?
Generally not.
It may be advisable to request a pelvic x-ray if an underlying pathology is suspected (for example, Developmental Dysplasia of the Hip, DDH).
Torsional CT and MRI must be requested by a specialist and only in very specific cases, mostly in preparation for surgical interventions.
Natural history: How will femoral anteversion evolve?
Children with excessive femoral anteversion show a progressive and spontaneous improvement with growth , up to approximately 10-12 years of age, which corresponds to the physiological development curve mentioned above.
In most cases, this improvement will lead to a complete resolution of the picture with a normalization of anteversion and gait.
In a percentage of children, femoral anteversion will persist to some extent but will be compensated for by the development of tibial external torsion. This results in a normalization of the gait angle (i.e., internal rotation is no longer present) with a partial misalignment (more or less pronounced) between the femur and tibia.
In a small percentage of children (about 20%, especially those who present with marked anteversion from the outset), the anteversion improves but persists (to a greater or lesser extent) once skeletal maturity is reached.
What does the possible persistence of femoral anteversion entail once skeletal maturity has been reached?
No study has ever demonstrated an association between excessive femoral anteversion and hip or knee osteoarthritis. Only in cases where excessive femoral anteversion and excessive tibial external torsion are combined at the end of growth can the subject theoretically be more susceptible to patellar problems.
Treatment of femoral anteversion
No specific treatment is necessary in most cases. Families should be reassured that this is a problem that will improve spontaneously and, even if it persists, will in almost all cases not cause any problems.
Braces, insoles, orthopedic shoes, physiotherapy or restrictions in sitting postures do not appear to alter the natural history of the problem.
Surgical treatment for severe femoral anteversion
Surgical treatment (femoral derotation osteotomy) is considered in very selected cases: in those older children (over 10 years old) in whom a very pronounced inward-pointing gait persists, causing significant functional impairment in daily life and in sporting activities.
In these cases of severe femoral anteversion, surgical treatment provides good results.
Find examples of cases treated for severe femoral anteversion in the “Clinical Cases” section.
Referral to a specialist is recommended in case of:
- Marked asymmetry in hip rotations and gait (one limb rotates inward a lot, the other does not)
- Pain, lameness
- Suspected underlying hip pathology
- Suspected underlying neurological pathology
- In older children (over 10 years) with persistent marked anteversion
ESSENTIAL BIBLIOGRAPHY:
- Blackmur JP, Murray AW: Do children who in-toe need to be referred to an orthopedic clinic? J Pediatr Orthop B19:415, 2010
- Fabry G, MacEwen GD, Shands AR Jr: Torsion of the femur. A follow-up study in normal and abnormal conditions, J Bone Joint Surg Am55:1726, 1973.
- Staheli LT: Torsion—treatment indications, Clin Orthop Relat Res 247:61, 1989.
- Staheli LT. Rotational problems in children. Instr Course Lect 1994;43:199-209.
- Rerucha CM, Dickison C, Baird DC. Lower Extremity Abnormalities in Children. Am Fam Physician. 2017 Aug 15;96(4):226-233.