
Arthrogryposis at birth: what to do?
If arthrogryposis is diagnosed at birth, it will be necessary to immediately make the diagnostic assessment and treatment (physiatric/orthopedic) proceed hand in hand: see dedicated sheet.
The treatment plan will be developed by a multidisciplinary team, whose ultimate goal will be to increase the patient’s independence, focusing not only on walking and mobility, but also on communication skills and activities of daily living. This plan will vary depending on the underlying condition (amyoplasia, distal arthrogryposis, forms with neurological involvement, etc) and the specific features of the individual patient.
To this end, assessments of joint deformities (dislocations, subluxations), contractures, and the patient’s muscle potential will be performed.
Orthopedic treatment of children with arthrogryposis will include:
- Physiotherapy plays a key role and should be started very early after birth. Stretching and joint mobilization should be taught to families and continued at home.
- thermoplastic splints
- orthoses : from simple insoles to AFO braces, to KAFO braces, to the more complex HKAFO (with pelvic extension) depending on the deformities and functional capabilities of the patient
- orthopedic shoes
- Serial casts
- Surgery (upper limb, spine, lower limb)
Arthrogryposis: surgical treatment
Below we provide a brief overview of the surgical treatment of the lower limbs in children with arthrogryposis.
One of the main difficulties in this area, besides the resistance to treatment of individual joint areas, is establishing a treatment sequence. Indeed, problems coexist at multiple levels and bilaterally, and these can hinder treatment of other joints. A great deal of experience is required to establish an appropriate treatment plan.

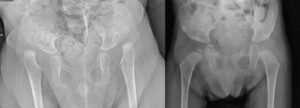
Hip surgery for arthrogryposis
Approximately 80% of children with classic arthrogryposis exhibit hip involvement, ranging from contracture of the soft tissue (tendons, capsules) to dislocation (unilateral or bilateral). Surgical interventions may include, depending on the case:
- soft tissue release, after failure of an adequate period of stretching
- Reduction of unilateral hip dislocations: This procedure is always recommended to symmetrically maintain the pelvis (for static purposes but also for sitting). It usually requires surgical reduction (open).

- Reduction of bilateral hip dislocations. There is controversy among various authors regarding the appropriateness of reduction in these cases. It is advisable to weigh the benefits (reduction can increase the patient’s ambulation potential) and risks (necrosis of the femoral heads, stiffness, recurrence, and the need for multiple interventions). In any case, it is advisable to perform the reductions at different times, given the perioperative risks associated with each individual procedure (bleeding, etc.).
- bone procedures (femoral osteotomies, pelvic osteotomies)

All interventions must be followed by adequate re-education periods and appropriate braces.
Knee surgery in arthrogryposis
Knee deformities are present in approximately 70% of children with classic arthrogryposis , presenting with flexion or extension deformities.

Knee flexion deformity in arthrogryposis
For flexion deformities, interventions may include:
- release of the soft tissues (hamstrings, posterior capsule) followed by possible progressive gypsotomies, i.e. progressive corrections in plaster using corrective stages
- distal femoral extension osteotomies
- gradual corrections with Ilizarov external fixator
- progressive corrections with anterior epiphysiodesis of the distal femur. These procedures have been used more frequently in recent years for these conditions, but their efficacy is still uncertain.
- In cases where cutaneous pterygia are present , collaboration with plastic surgeons is useful to treat both the skin component and the joint deformity component.

Knee extension deformity in arthrogryposis
For extension deformities (recurvatum, subluxation, dislocation), possible interventions include, after an adequate period of non-surgical treatment:
- quadricepsplasty using an inverted V-shaped anterior approach
- anterior capsulotomy with reduction of dislocation
Foot surgery in arthrogryposis
Foot deformities are common in all forms of arthrogryposis, and particularly in amyoplasia and the distal forms.
The most common forms are congenital clubfoot equinovarus and congenital vertical talus; equinus deformities are rarer.

For the equinovarus foot , the interventions include, depending on the patient’s age, the severity of the deformity and previous treatments:
- Ponseti method: correction using progressive casts. The results obtained are inferior to those achieved with idiopathic clubfeet. Specifically, the percentage of feet that cannot achieve complete correction and require surgical release is higher (and this occurs more frequently in amyoplasia and less frequently in distal arthrogryposis), and the recurrence rate is higher. For this reason, even after the deformity has been corrected, it is important to use both Ponseti and AFO braces for extended periods, combined with physiotherapy.
- extensive soft tissue release, with tendon resections
- osteotomies (Evans, Lichtblau, etc.)
- talectomies, which some authors indicate as primary treatment, but which in our opinion should be used with caution and should be reserved only as a last choice treatment in the foot that has already relapsed
- correction using the Ilizarov external fixator , which allows progressive corrections for the most severe and complex deformities
For forms of congenital vertical talus, the following are indicated, after initial non-invasive treatment/Ponseti method:
- soft tissue release (medial, posterior and lateral) with reduction of dislocations
- corrective osteotomies, talectomies, Grice procedure
- double/triple arthrodesis once skeletal maturity has been reached, in the case of recurrence/incomplete correction
In any case, the deformities tend to be rigid and resistant to treatment and have a high rate of recurrence, therefore periodic checks and adequate support (insoles, AFO braces, orthopedic footwear) will be necessary.

For further information, please refer to the scientific works:
- Management of knee deformities in children with arthrogryposis. Lampasi M, Antonioli D, Donzelli O. Musculoskelet Surg. 2012 Dec;96(3):161-9.
- Management of hip contractures and dislocations in arthrogryposis. Stilli S, Antonioli D, Lampasi M, Donzelli O. Musculoskelet Surg. 2012 Jun;96(1):17-21.